.svg)
BPSD: What it means, how it's assessed, and how to manage it at home
BPSD affects up to 90% of people with dementia. Discover the causes, assessment tools, and evidence-based strategies for managing symptoms at home.
Author: Sensible Care

BPSD stands for behavioural and psychological symptoms of dementia. It refers to the emotional and behavioural changes that occur alongside the cognitive decline of dementia. These include agitation, depression, anxiety, and apathy. These symptoms arise from a mix of brain changes, physical health issues, and environmental factors. Non-pharmacological approaches like structured routines, music therapy, and carer education can help. Support services are available across Australia for both people living with dementia and their carers.
BPSD stands for behavioural and psychological symptoms of dementia. These are non-cognitive symptoms, including agitation, depression, anxiety, apathy, and hallucinations. These symptoms occur alongside the memory and thinking changes of dementia.
Up to 90% of people with dementia experience BPSD at some point during their illness. In Australia, that represents a significant part of the estimated 433,300 people currently living with dementia.
What does BPSD mean in dementia?
BPSD refers to the emotional, behavioural, and perceptual changes that arise from the brain changes caused by dementia. These symptoms are not deliberate or wilful. They reflect how a damaged brain processes and responds to the world.
BPSD is sometimes called the neuropsychiatric symptoms of dementia. The two terms refer broadly to the same cluster of changes. Clinicians use both, but "BPSD" is the most common shorthand in Australian aged care.
These symptoms affect quality of life just as significantly as memory loss. They are also a leading cause of entry into residential aged care and a major source of distress for family carers.
What are the most common BPSD symptoms?
The five most common BPSD symptoms are:
- Apathy
- Depression
- Anxiety
- Irritability
- Agitation or aggression
These appear across all dementia types, though the mix varies by diagnosis.
Source: Kwon & Lee, 2021
A 1999 study by Frisoni found that half of all people with dementia experience at least four neuropsychiatric symptoms at the same time. This means BPSD rarely manifests as a single, isolated behaviour.
Some people with dementia also experience sundowning. This is increased confusion, agitation, or restlessness that occurs in the late afternoon or evening.
How BPSD differs by dementia type
The type of dementia shapes which symptoms are most prominent. According to a 2021 study by Kwon and Lee, agitation and aggression affect 53% of people with frontotemporal dementia. Anxiety affects 51%. In Alzheimer's disease, apathy and depression tend to dominate.
Neuropsychiatric symptoms are present in 56–98% of cases in people with dementia living at home. According to a 2012 study by Cerejeira et al., the rate rises to 91–96% in residential aged care. This gap reflects both the severity of dementia in aged care settings and the role that the environment plays in behaviour.
How is BPSD assessed?
BPSD is assessed using structured tools that measure a range of symptom characteristics.
The most widely used tool in Australian aged care is the Neuropsychiatric Inventory (NPI). It scores each symptom domain based on frequency and severity. The NPI also includes a separate scale, rating the distress experienced by the carer.
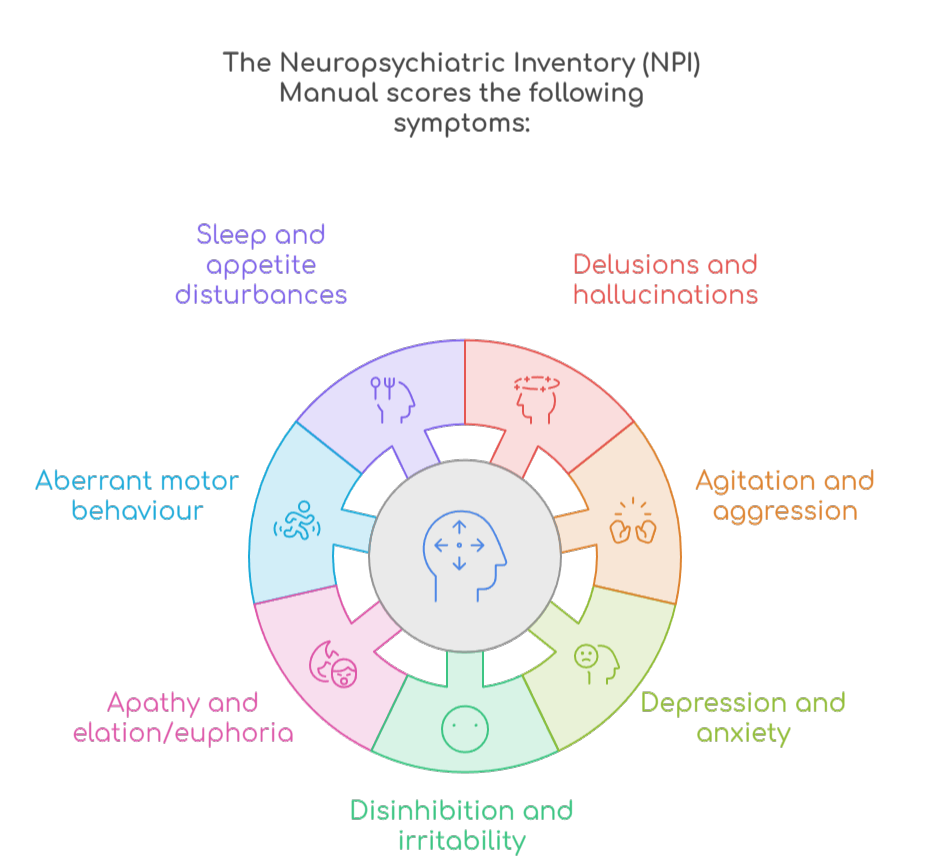
The Neuropsychiatric Inventory (NPI) Manual was developed by Dementia Training Australia in 2016. According to the manual, the NPI covers ten behavioural and two neurovegetative domains, for a total of twelve symptom areas. These include:
- Delusions and hallucinations (how often the person holds false beliefs or sees, hears, or feels things that are not there)
- Agitation and aggression (restless, resistive, or physically aggressive behaviour)
- Depression and anxiety (persistent low mood and excessive worry, fear, or tension)
- Apathy and elation/euphoria (loss of motivation or interest, and episodes of unusually elevated or expansive mood)
- Disinhibition and irritability (socially inappropriate or impulsive behaviour and short temper)
- Aberrant motor behaviour (repetitive purposeless movements such as pacing or rummaging)
- Sleep and appetite disturbances (disrupted sleep–wake patterns and changes in eating habits)
For each domain, a carer rates the symptom across two dimensions:
Frequency (how often the symptom occurs):
- 1 = rarely
- 2 = sometimes
- 3 = often
- 4 = very often
Severity (how intense the symptom is):
- 1 = mild
- 2 = moderate
- 3 = severe
The domain score is calculated by multiplying frequency by severity. Carers also rate their own distress on a six-point scale, from 0 (not at all distressing) to 5 (very severely distressing).
What structured assessment adds
A structured assessment does more than name symptoms. It identifies triggers, patterns, and the timing of behaviours. It also captures carer distress, which is itself a strong predictor of whether community care can continue.
Good assessment practice includes reviewing recent changes in health, medications, and routine. It also screens for reversible causes before attributing a behaviour to dementia progression. These include pain, infection, delirium, and sensory impairment.
What causes BPSD?
BPSD arises from a mix of brain changes, medical factors, psychological history, and environment. It doesn't stem from dementia pathology alone. Understanding these causes determines how you respond.
Neurological causes
BPSD can result from damage to the brain circuits that regulate emotion and behaviour. Different dementia types damage different circuits, which is why symptom profiles vary.
Medical and physical causes
Medical and physical causes of BPSD include pain, constipation, urinary retention, infection, and medication side effects. These causes are reversible. Missing them leads to unnecessary distress and inappropriate treatment.
Environmental and psychosocial causes
Environmental and psychosocial causes of BPSD include:
- Noise
- Poor lighting
- Disrupted routines
- Overcrowding
- Lack of meaningful activity
A person with dementia has a reduced capacity to interpret and adapt to a demanding environment. When the environment becomes too much to process, that distress often manifests as behaviour.
Current best practice recognises that BPSD is often a sign of unmet need, not wilful behaviour. A person who is agitated may be in pain, frightened, bored, or overstimulated. Understanding this shifts the focus from managing behaviour to finding out what's behind it.
Creating a dementia-friendly home environment
The physical environment has a direct impact on BPSD. A home that is calm, familiar, and easy to navigate reduces sensory overload. Small, practical changes can make a significant difference, which apply to:
- Lighting
- Noise and overstimulation
- Familiarity and cues
- Cluster and safety
- Outdoor access
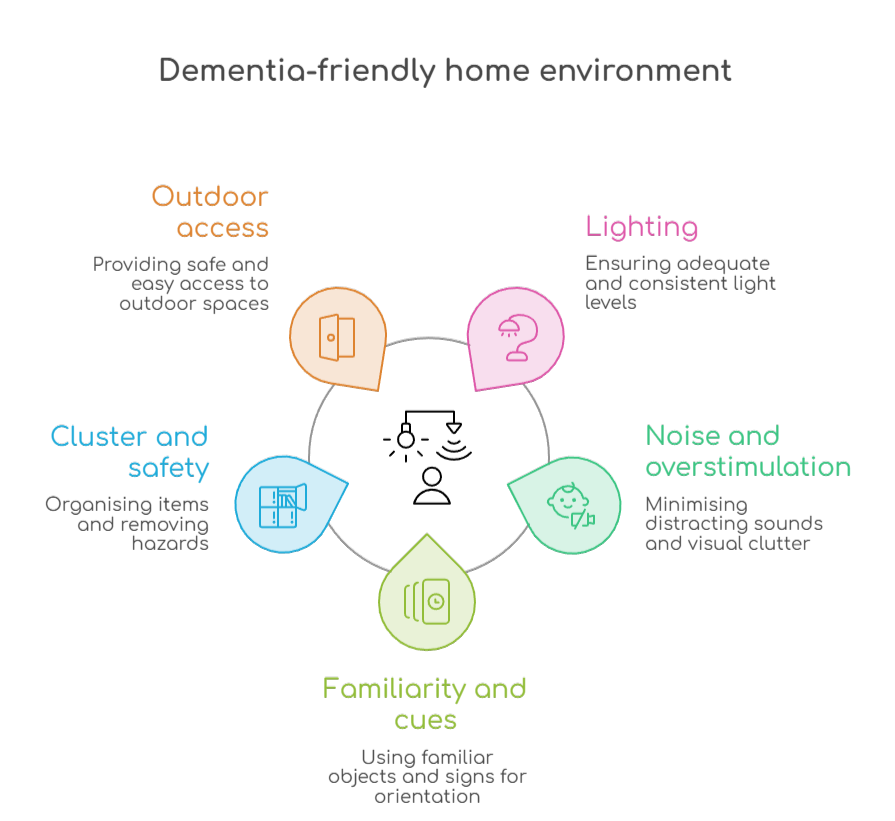
Keep living areas well-lit during the day to support orientation and reduce shadows, which can cause misperceptions or fear. Use nightlights in hallways and bathrooms to reduce confusion and fall risk after dark.
Limit background noise from televisions, radios, or multiple conversations happening at once. A quieter environment reduces the cognitive load on a person with dementia and lowers the likelihood of agitation.
Keep furniture arrangements consistent and display familiar objects, photographs, and meaningful items. Predictable surroundings help the person feel safe and oriented. Clear labels on cupboards and doors can support independence and reduce frustration.
Remove unnecessary clutter from floors and surfaces to reduce confusion and fall risk. Lock away medications, cleaning products, and sharp objects where needed.
Where safe, access to a garden or outdoor space supports mood, reduces apathy, and provides gentle physical activity.
What are the non-pharmacological approaches to BPSD?
Non-pharmacological approaches are the first-line treatment for BPSD in Australia. They include personalised activities, music therapy, environmental changes, carer education, and structured routines.
Australia's Dementia Behaviour Management Advisory Service (DBMAS) and Severe Behaviour Response Teams (SBRT) deliver structured psychosocial programmes. A 2021 evaluation by Caplan et al. found NPI scores dropped by 61.4% (DBMAS) and 74.3% (SBRT). Carer distress scores fell by 66.5% and 69.1%, respectively.
Carer support as a core strategy
Carer support is a core part of BPSD management. The presence and frequency of BPSD are strongly linked to carer strain, depression, and physical health problems. Carers who receive education and practical skills training show measurable reductions in distress.
Keeping a diary of when and where behaviours occur helps identify triggers. Dementia Australia's National Dementia Helpline (1800 100 500) is available 24 hours a day, seven days a week, 365 days a year.
When is medication used for BPSD?
Medication is used for BPSD only when symptoms are severe, pose a safety risk, and have not improved with other approaches. It is not a first-line or routine response.
Antipsychotics carry serious risks in people with dementia. A 2009 study by Andrade and Radhakrishnan found that antipsychotic drugs increase the risk of stroke-related events by 70%. Atypical antipsychotics are also linked to a 31–55% higher mortality rate compared to no antipsychotic use.
A 2019 study by Lind et al. found that up to a third of aged care residents with dementia were prescribed antipsychotics each year. Of those, 65% were on antipsychotics for more than three months, even without a psychiatric diagnosis.
Concerns about overprescribing in Australian aged care had been raised for decades. This prompted government inquiries, prescribing restrictions, and targeted interventions.
One such intervention was the Australian RedUSe programme. According to a 2018 study by Westbury et al., the program reduced antipsychotic prescribing by 13% and benzodiazepine prescribing by 21% within six months.
In that program, 39% of residents who were prescribed these drugs at baseline had them ceased or reduced. This outcome was achieved within six months.
Does BPSD occur in people living at home?
BPSD occurs commonly in people living at home, not only in residential aged care. A 2012 study by Cerejeira et al. found that neuropsychiatric symptoms occur in 56–98% of people with dementia living in the community. Many families encounter BPSD long before residential care is considered.
According to Dementia Australia, one in three people with dementia lives in residential aged care. That means two in three people with dementia live at home or in the community. For most families, that means managing behavioural changes at home.
A 2025 study by Atee et al. found that BPSD contributes to roughly 30% of total dementia care costs. Unmanaged symptoms speed up the transition from home to residential care.
What support is available in Australia for BPSD?
Australia funds several programs for people with BPSD and their carers, including:
- Dementia Support Australia (DBMAS and SBRT)
- The Specialist Dementia Care Program
- Government‑subsidised home support (formerly Home Care Packages, now the Support at Home program under the new Aged Care Act)
- NDIS funding for people with younger‑onset dementia
Dementia Support Australia (DBMAS and SBRT)
Dementia Support Australia provides free assessment and short-term case management. Both people with BPSD in the community and residential care can use it.
Their DBMAS and SBRT programs are government-funded. According to a 2021 evaluation by Caplan et al., they achieved NPI reductions of 61.4% and 74.3%, respectively.
Specialist Dementia Care Programme (SDCP)
People with BPSD can also use the Specialist Dementia Care Programme. It provides small, dementia-friendly residential units for people with very severe BPSD. The goal is to stabilise behaviour before transitioning people to less intensive care.
Support at Home
The Support at Home program funds coordinated in‑home support for older people, including those living with dementia. Funding can cover personal care, domestic help, nursing, allied health, and other supports delivered in the home. These supports can include dementia‑specific services.
NDIS for younger-onset dementia
According to Dementia Australia, an estimated 29,000 Australians were living with younger‑onset dementia in 2025. If they meet the eligibility requirements, people with younger‑onset dementia may access the NDIS for:
- Capacity‑building supports
- Personal care
- Community participation
This can include support for managing the behavioural and psychological impacts of dementia.
FAQ
Is BPSD the same as dementia?
BPSD is not the same as dementia, but it is part of it. Dementia is diagnosed based on cognitive decline and loss of function.
BPSD refers to the behavioural and emotional symptoms that occur alongside cognitive decline. These can include agitation, depression, anxiety, and apathy.
Not everyone experiences the same BPSD symptoms. Their severity varies widely between individuals.
Can BPSD be prevented or reduced at home?
Many BPSD symptoms can be reduced. This is possible through consistent routines, meaningful activities, and a calm sensory environment.
Identifying and addressing triggers helps prevent escalation. These triggers can include pain, boredom, noise, or disrupted sleep.
Specialist programs provide free in-home assessment and support for families managing difficult behaviours.
Are antipsychotic medications safe for people with dementia?
According to a 2009 study by Andrade and Radhakrishnan, antipsychotic medications carry serious risks for people with dementia. This includes a 70% increased risk of stroke-related events and a 31–55% higher mortality rate compared to no antipsychotic use.
Australian guidelines reserve antipsychotics for severe symptoms that haven't responded to other approaches. They should be used at the lowest dose for the shortest time possible.
When should I seek specialist help for BPSD?
Seek specialist help when behaviours are causing significant distress or placing safety at risk. It's also worth reaching out if symptoms are not improving with the strategies already in place.
Dementia Support Australia's DBMAS helpline (1800 699 799) offers free, confidential expert advice. The National Dementia Helpline (1800 100 500) operates 24/7 and can connect you with the right support.
Does BPSD only happen in advanced dementia?
No. BPSD can occur at any stage of dementia, including in the earlier stages. A 2012 study by Cerejeira et al. confirms this. It found that neuropsychiatric symptoms are present in 56–98% of people with dementia living in the community.
Agitation, depression, anxiety, or apathy can occur well before dementia is advanced. Seeking help early makes it easier to identify triggers and put the right supports in place.
Managing BPSD takes the right support
BPSD is a normal part of dementia for most people, but it doesn't have to be managed alone. Understanding what drives behavioural and psychological symptoms is the first step. The right strategies can make a meaningful difference for both the person living with dementia and those who care for them.
If you're supporting someone at home who is experiencing BPSD, Sensible Care can help. Our in-house allied health team delivers personalised assessment and support directly in the home. We accept 8+ government funding types, including Support at Home and NDIS.
There are no lock-in contracts, no daily fees, and no exit charges. Call us today to book a free initial consultation.
Take the Next Step in Care
Download our Info Kit or speak to one of our friendly team members today.
Explore More Helpful Reads
More stories, guides, and updates to support you and your family.



Need Help Getting Started?
Reach out on your terms, pick a time that suits you and let’s talk about how we can help.
.webp)